A Complete Medical & Practical Guide — Evidence-Based
Medically Reviewed by Dr. V.N. Bharti, Sexologist (16+ years experience) | Last Updated: May 2026
| MEDICAL DISCLAIMER:This article is for informational purposes only. Always consult a qualified healthcare professional for diagnosis and treatment. |
Before We Begin: You Are Not Alone
If you have clicked on this article, you have probably already spent time worrying — quietly, alone — about something that feels too personal to raise with anyone else. Premature ejaculation carries a weight that goes far beyond the bedroom. It chips away at confidence, fuels dread before intimacy, and can make a man feel broken in a way that is hard to articulate.
Here is what we want you to know from the very first line: you are not broken. PE affects roughly 1 in 3 men at some point in their lives. It is a recognised medical condition with well-understood causes and a very high rate of successful treatment.
| “Many men wait years — sometimes decades — before seeking help. In Dr. Bharti’s clinic, the turning point is almost always the same: the moment a man realises this is treatable.” |
This guide covers everything — from what PE is and why it happens, to a proprietary recovery framework developed from 16+ years of clinical practice. It is written to be both medically authoritative and humanly readable.
How to Use This Guide
This is a long, comprehensive pillar article — use the quick navigation below to jump directly to what matters most to you right now. Every section is self-contained.
| QUICK NAVIGATION |
| → Section 1: What Is PE? |
| → Section 2: Types of PE |
| → Section 3: Symptoms & Self-Diagnosis |
| → Section 4: Causes |
| → Section 5: PE vs. Erectile Dysfunction |
| → Section 6: Mental Health & Relationships |
| → Section 7: When to See a Doctor |
| → Section 8: Clinical Diagnosis |
| → Section 9: Treatment Overview |
| → Section 10: 7 Techniques to Last Longer |
| → Section 11: Kegel Exercises (12-Week Plan) |
| → Section 12: Lifestyle Changes |
| → Section 13: Performance Anxiety |
| ★ Section 14: Dr. Bharti’s 4-Stage Recovery Framework |
| → Section 15: FAQs |
| → Section 16: Entity Glossary & Further Reading |
| → Section 17: References |
What You Need to Know in 60 Seconds
| PE is the most common male sexual dysfunction, affecting 1 in 3 men globally. |
| Clinical definition: ejaculation within 1 minute of penetration (ISSM, 2014), with distress. |
| PE is highly treatable — with behavioural techniques, Kegels, topical agents, or medication. |
| Ask yourself: Do I ejaculate within 1-2 minutes more than 50% of the time? |
| Is this causing distress, frustration, or affecting my relationship? |
| If yes — this guide will show you the path forward. |
1. What Is Premature Ejaculation?
Premature ejaculation (PE) is a male sexual dysfunction characterised by ejaculation that occurs sooner than desired — before or very shortly after penetration — causing personal distress or interpersonal difficulty. It is the most prevalent male sexual complaint worldwide (Laumann et al., 1999, JAMA).
The International Society for Sexual Medicine (ISSM, 2014) provides the most widely accepted clinical definition:
| Criterion | Clinical Threshold |
| Intravaginal Ejaculatory Latency Time (IELT) | Less than 1 minute from penetration |
| Pattern | Always or nearly always |
| Control | Inability to delay ejaculation on all or nearly all occasions |
| Distress | Negative personal consequences — anxiety, frustration, avoidance |
| Duration | Lifelong OR since a specific change (acquired) |
In plain English: if you consistently finish before you want to and it bothers you — that is PE. The clinical criteria simply make this precise enough to diagnose and treat.
| Reassurance |
| Occasional early ejaculation during stress, new partners, or long abstinence is NOT clinical PE. PE requires a persistent pattern plus genuine distress. You are not ‘broken’ — PE is a recognised, highly treatable medical condition. |
2. Types of Premature Ejaculation
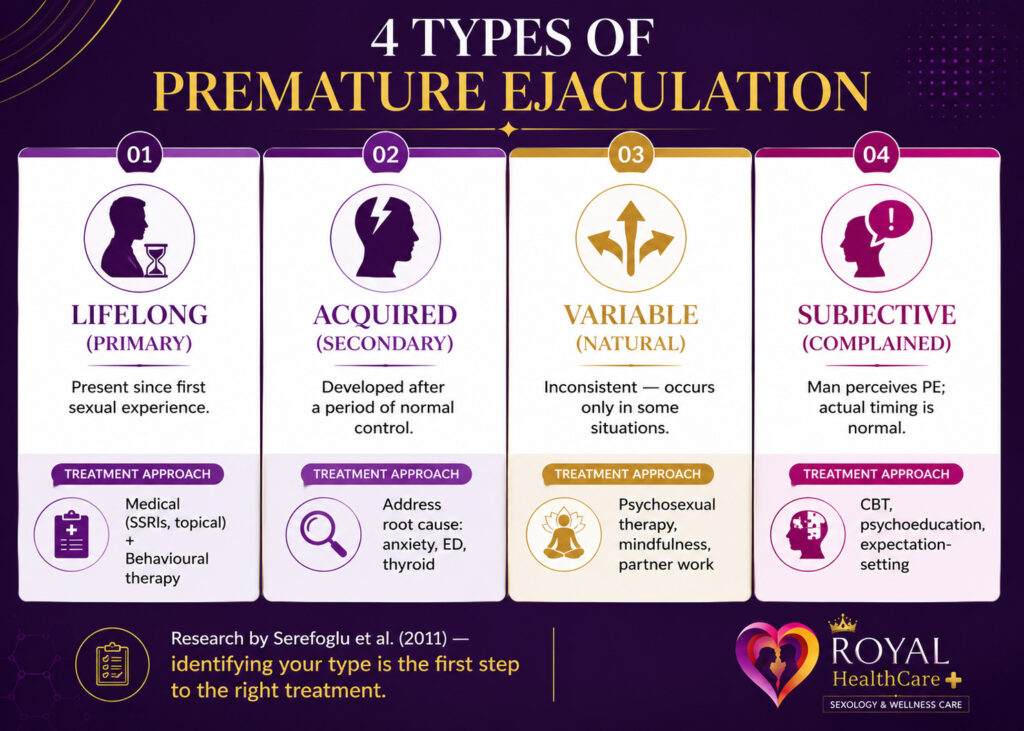
Research by Serefoglu et al. (2011) identified four clinically distinct PE subtypes. Understanding your type is the first step toward selecting the right treatment.
| Type | Definition | Best Treatment Approach |
| Lifelong (Primary) | PE present since first sexual experience | Medical (SSRIs, topical) + Behavioural therapy |
| Acquired (Secondary) | PE developed after normal ejaculatory control | Address underlying cause (anxiety, ED, thyroid) |
| Variable (Natural) | Inconsistent — occurs in some situations only | Psychosexual therapy, mindfulness, partner work |
| Subjective (Complained) | Man perceives PE; actual timing is normal | CBT, psychoeducation, expectation-setting |
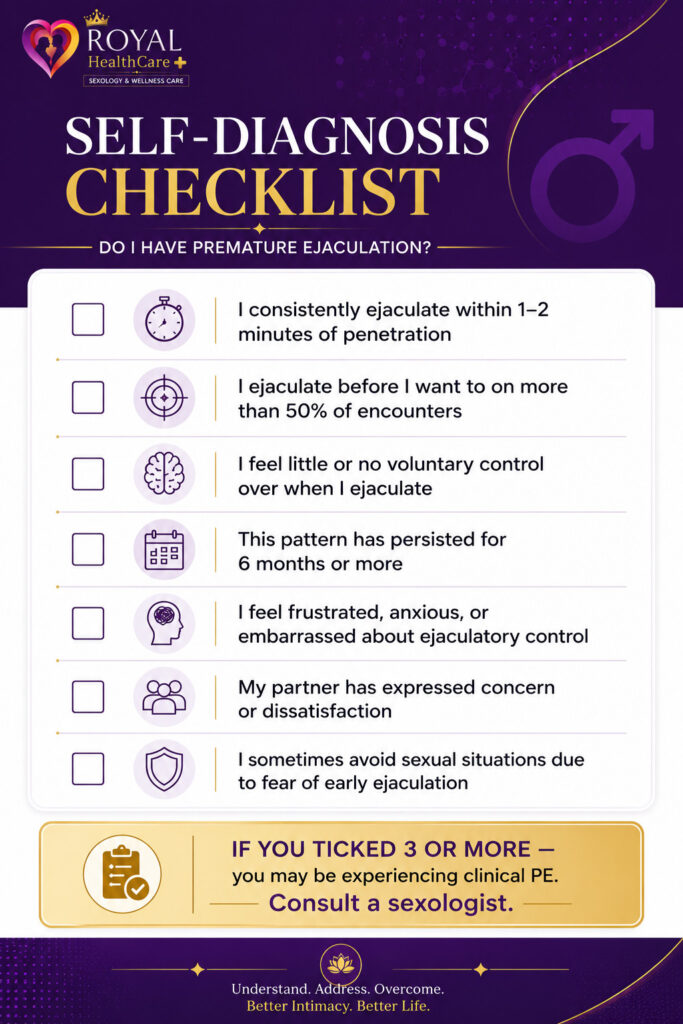
3. Symptoms & Self-Diagnosis
Use the structured checklist below for a first self-assessment.
Understanding Your IELT
IELT — Intravaginal Ejaculatory Latency Time — is simply the clock time from penetration to ejaculation. It is the gold-standard clinical measure.
Think of IELT as your body’s ‘response time.’ The median for most men is about 5-6 minutes. Men with PE typically clock under 1 minute — but this response time can be trained and extended.
- IELT below 1 minute = consistent with PE diagnosis (ISSM criteria)
- IELT 1-2 minutes = borderline; distress determines clinical significance
- IELT above 2 minutes = usually not classified as PE unless significant loss of control is perceived
4. Causes of Premature Ejaculation
PE is rarely caused by a single factor. Research identifies a combination of psychological, physical, neurological, and lifestyle contributors.
| Psychological | Physical / Hormonal | Neurological | Lifestyle |
| Performance anxiety* | Hyperthyroidism (50-70% of hyperthyroid men report PE) | Penile hypersensitivity (hyperactive ejaculatory reflex) | Excessive alcohol use |
| Early sexual conditioning (rushed masturbation) | Low serotonin levels | Dopamine dysregulation | Sedentary lifestyle |
| Depression or generalised anxiety disorder | Prostatitis | CNS hyperexcitability | Pornography-driven conditioning |
| Relationship conflict or poor communication | Erectile dysfunction (ED) — rushing before losing erection | Reduced inhibitory control in brainstem ejaculatory centres* | Poor sleep, chronic fatigue |
| History of sexual trauma or guilt | Testosterone imbalance | Spinal cord hypersensitivity | High-stress occupation |
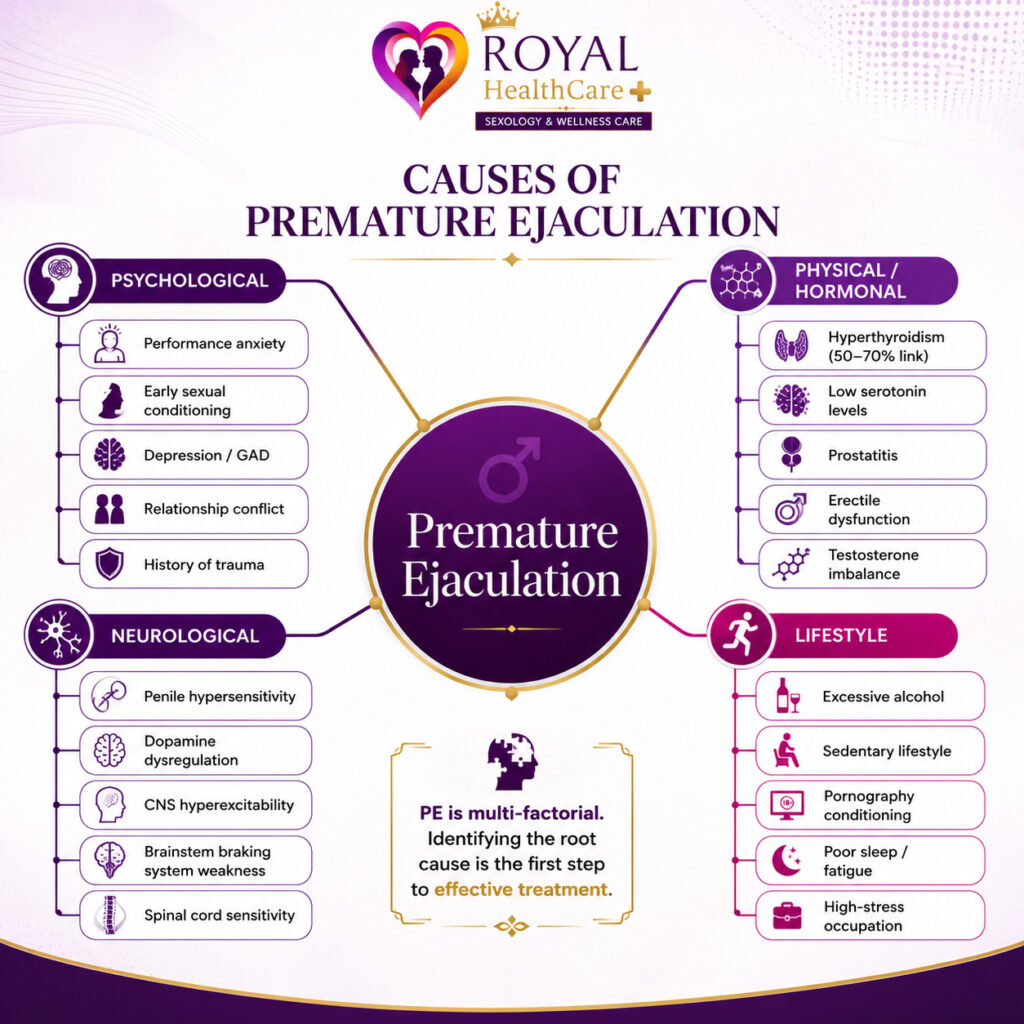
* The brainstem ‘braking system’ for ejaculation becomes less effective — making it harder to slow down once arousal builds. The good news: this can be retrained.
“Performance anxiety is the #1 psychological trigger for acquired PE — and it creates a self-fulfilling cycle. The fear of ejaculating quickly causes the very outcome it fears.”
5. PE vs. Erectile Dysfunction
PE and erectile dysfunction (ED) are frequently confused — and they can co-exist. Understanding the difference is critical for the right diagnosis and treatment.
| Feature | Premature Ejaculation (PE) | Erectile Dysfunction (ED) |
| Core problem | Ejaculates too quickly | Cannot achieve or maintain erection |
| Erection quality | Usually normal | Impaired or absent |
| Timing | At or shortly after penetration | Before or during penetration |
| Primary emotion | Embarrassment, lack of control | Shame, performance pressure, depression |
| Can they co-exist? | Yes — PE can trigger ED via anxiety | Yes — ED can cause PE (rushing to climax) |
| Main treatments | Behavioural techniques, SSRIs, topical agents | PDE5 inhibitors, lifestyle changes |
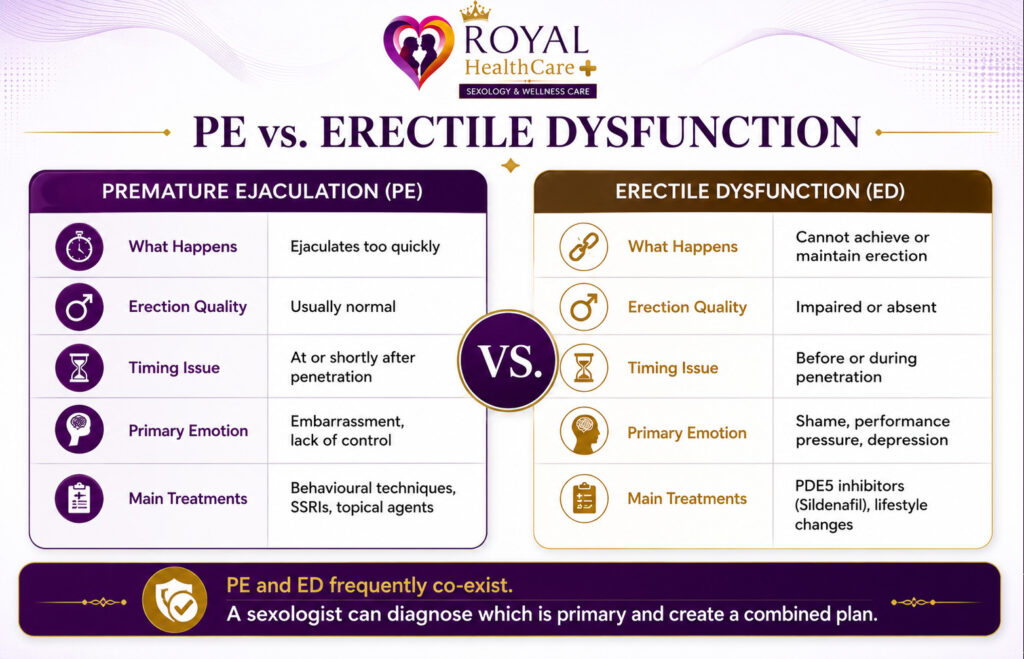
| Clinical Note |
| If you experience both PE and ED simultaneously, seek professional evaluation. A sexologist can determine which condition is primary and structure a combined treatment plan. |
6. How PE Affects Mental Health & Relationships
The psychological impact of PE is frequently underestimated. Far from being purely physical, PE erodes self-esteem, creates relationship tension, and can spiral into avoidance and depression.
The Emotional Toll on Men
- Chronic shame and embarrassment about sexual performance
- Avoidance of new sexual relationships or intimacy
- Reduced masculine self-image and daily confidence
- Secondary depression triggered by persistent frustration
- Hypervigilance during sex — monitoring performance rather than being present
| Patient Story — Vikram, 28 |
| “I’d been with my girlfriend for two years. She never complained — but I could tell she was unsatisfied. I started making excuses to avoid sex. Tired. Stressed. The truth was I was terrified. When I finally got help, I realised the anxiety was making everything worse. It was a loop I could not see from inside it.” |
| — Vikram, 28, marketing executive (name changed for privacy) |
Vikram’s avoidance pattern is one of the most common presentations in Dr. Bharti’s clinic. The anxiety-avoidance cycle feels impossible to break alone — but it responds very well to structured treatment.
How to Talk to Your Partner About PE
Choose a moment outside the bedroom, in a calm, private setting. Frame PE as a shared challenge, not a personal failure. Use ‘we’ language: ‘I’d like us to work through this together.’ Many couples report that honest conversation significantly reduces anxiety even before any formal treatment begins.
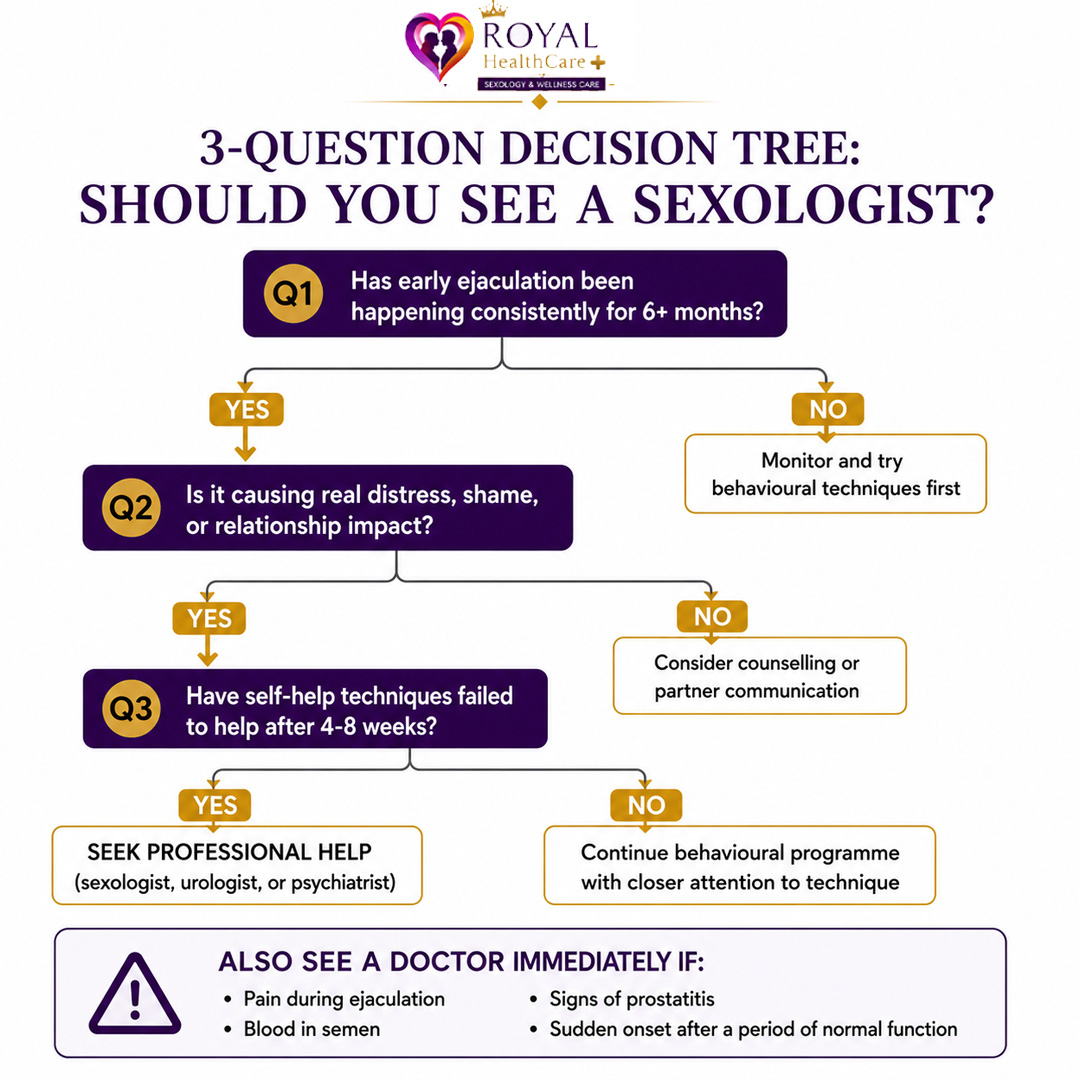
7. When Should You See a Doctor?
8. How PE Is Clinically Diagnosed
A sexologist will use patient history, validated questionnaires, and occasionally physical or blood tests to diagnose PE. Many men worry about judgment — in practice, sexual health specialists hear these concerns every day and are trained to make patients feel heard, not ashamed.
A common patient fear: ‘Will the doctor judge me?’ In clinical experience, the opposite is true. The appointment is a structured, non-judgmental conversation — rarely more than 45 minutes.
- Detailed sexual history: age of onset, IELT estimate, partner history, masturbation patterns
- Psychological screening: anxiety, depression, relationship stress (GAD-7, PHQ-9)
- Medical history: thyroid function, prostate health, medications, alcohol/drug use
- Validated questionnaire: Premature Ejaculation Diagnostic Tool (PEDT) or Index of Premature Ejaculation (IPE)
- Blood tests if indicated: thyroid function, testosterone, prolactin
9. Treatment Options — Full Overview
PE has one of the highest treatment success rates of any male sexual dysfunction. Combination approaches (behavioural + pharmacological) consistently outperform single modalities.
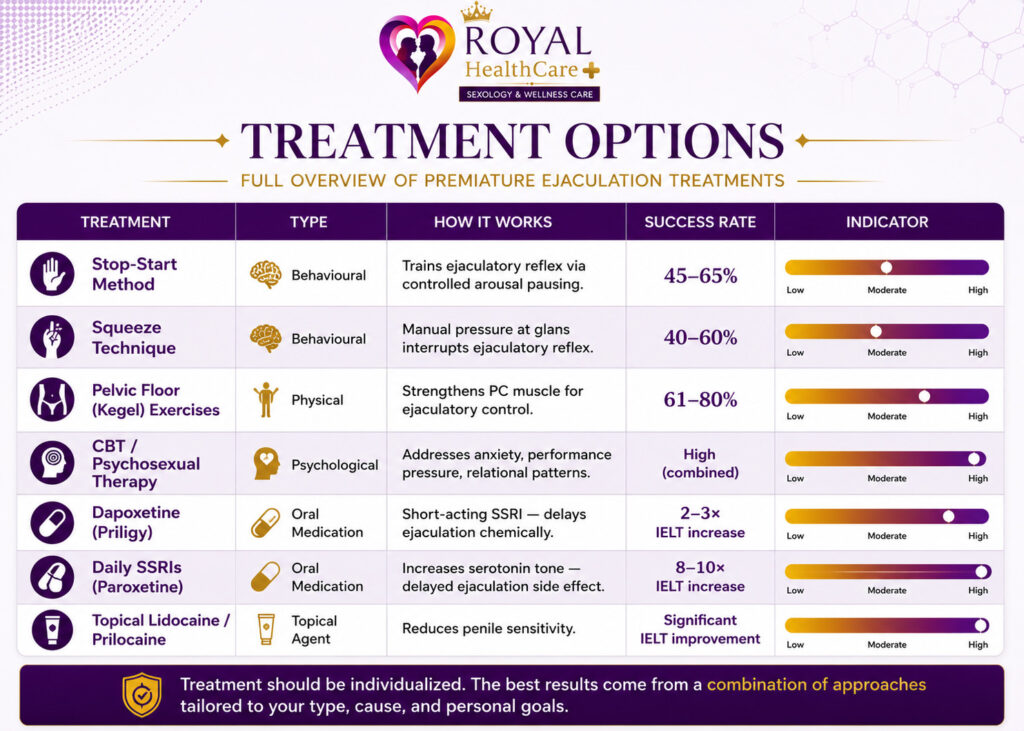
Note: All medications must be prescribed and supervised by a qualified doctor. Do not self-medicate.
10. 7 Techniques to Last Longer in Bed
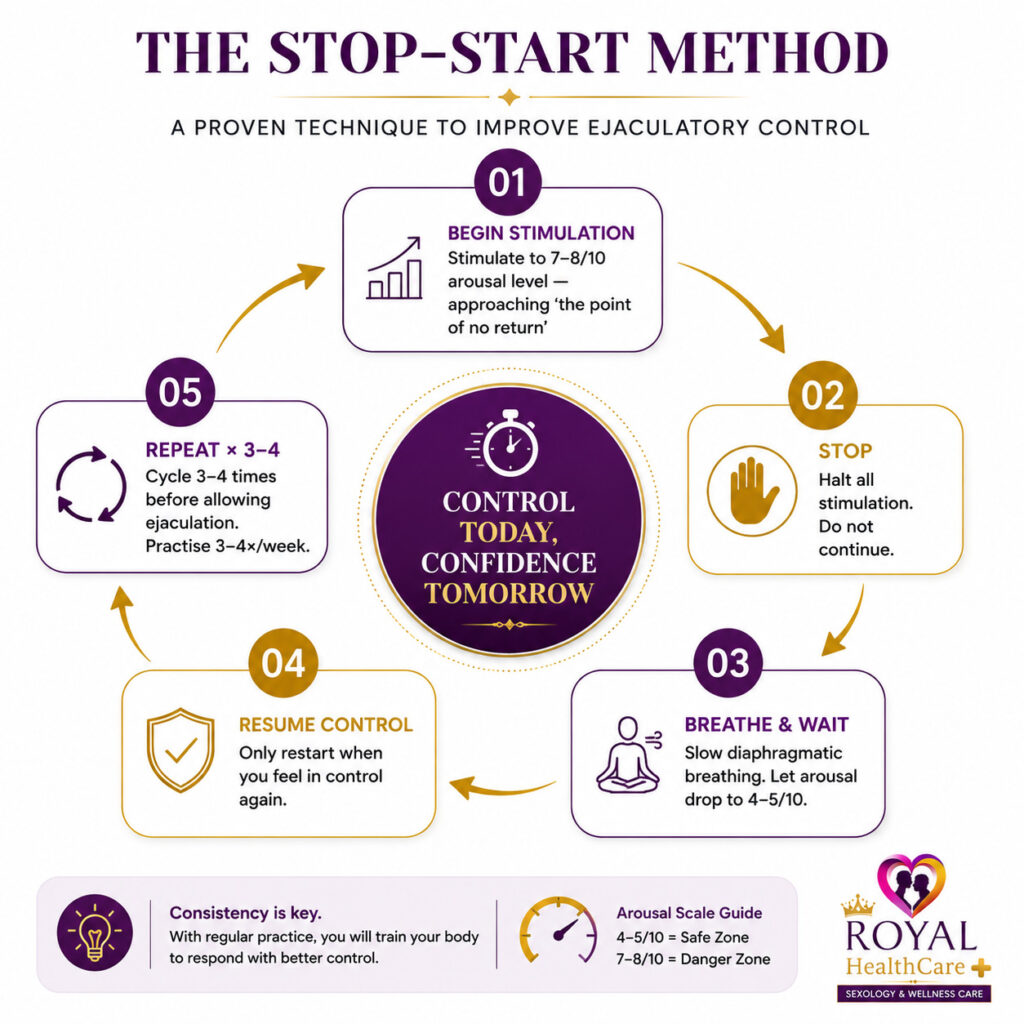
Technique 1: The Stop-Start Method
Originally described by Dr. James Semans in 1956, this trains the ejaculatory reflex through controlled arousal management. Success rate: 45-65%.
Think of it like strength training for your nervous system. The more you practise stopping at the edge of arousal, the more grip you develop over your ejaculatory response.
- Stimulate to 7-8/10 arousal (close to ‘the point of no return’ — but not at it)
- STOP all stimulation. Breathe slowly. Allow arousal to drop to 4-5/10.
- Resume once you feel in control. Repeat 3-4 times before allowing ejaculation.
- Practise 3-4 times per week; progress from solo to partnered intercourse over 4-6 weeks.
Technique 2: The Squeeze Technique
Developed by Masters & Johnson. Uses manual pressure to interrupt the ejaculatory reflex. Success rate: 40-60%.
This works by sending a ‘reset signal’ to the nervous system — essentially hitting a temporary pause button on the arousal cycle.
- Proceed to 7-8/10 arousal. Apply firm squeeze pressure at the head of the penis (glans/frenulum).
- Hold 10-20 seconds until the urge subsides. Wait 30 seconds, then resume. Repeat 3-4 times.
Technique 3: Deep Breathing & Mindful Awareness
Rapid, shallow breathing activates the sympathetic nervous system (‘fight or flight’) and accelerates ejaculation. Diaphragmatic breathing counteracts this.
A simple rule: if your breathing quickens, so does everything else. Slow your breath, and you slow the clock.
Practice: 4 seconds in, hold 2, 6 seconds out — sustained throughout intercourse.
Technique 4: Edging (Solo Arousal Training)
Repeatedly approach the edge of orgasm during masturbation and stop — over sessions of 20-30 minutes. This recalibrates the ejaculatory threshold upward.
Think of edging as raising the ceiling on your arousal. The higher your threshold, the longer you can stay below it during partnered sex.
Technique 5: Pelvic Floor Awareness & Relaxation
Many men unconsciously tighten their pelvic floor during sex — this reflexively triggers faster ejaculation.
Imagine gripping a steering wheel with white knuckles versus holding it lightly. A clenched pelvic floor accelerates the process. Learning to ‘let go’ mid-intercourse is a skill that takes practice but pays off significantly.
Technique 6: Sensate Focus
A sex therapy technique that shifts attention from performance to sensation. Couples take turns touching non-genitally first, then progressively move to full contact — removing the pressure of ‘lasting.’ Especially effective when PE is rooted in performance anxiety.
Technique 7: Positional Adjustment
Positions with the woman on top reduce muscular tension and allow better arousal regulation. Shallow thrusting reduces glans stimulation intensity. These are adjunct strategies — not standalone treatments, but useful immediate tools.
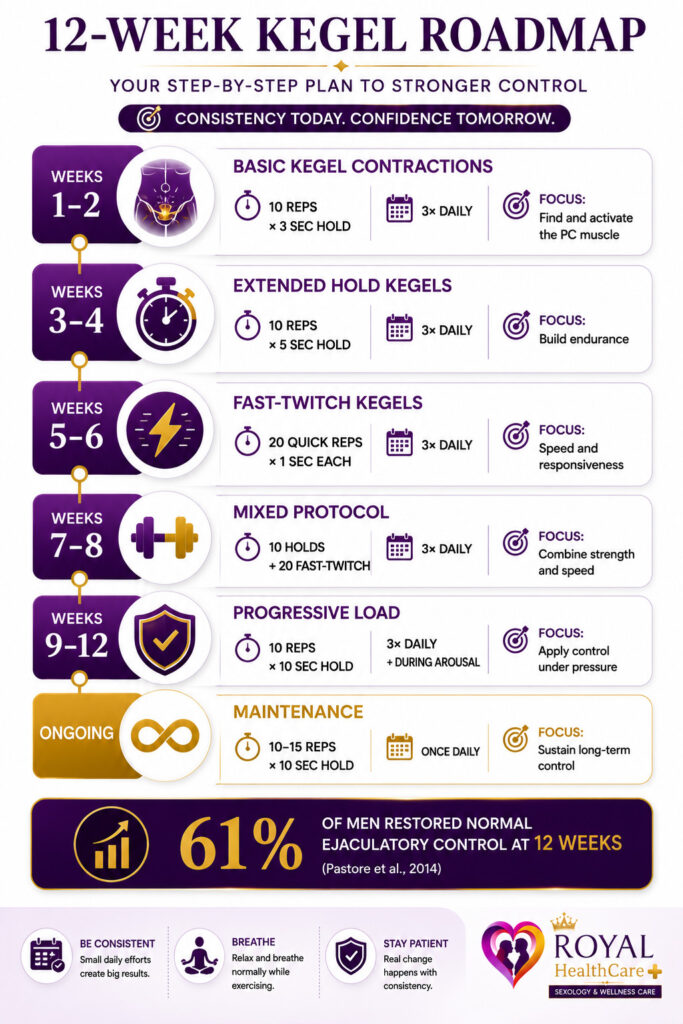
11. Pelvic Floor (Kegel) Exercises for Men — 12-Week Plan
A landmark RCT by Pastore et al. (2014) found that a 12-week pelvic floor programme restored normal ejaculatory control in 61% of men with lifelong PE, with a further 19% showing significant improvement.
“8 out of 10 men who completed the 12-week Kegel programme experienced meaningful improvement — no medication, no side effects, no cost.”
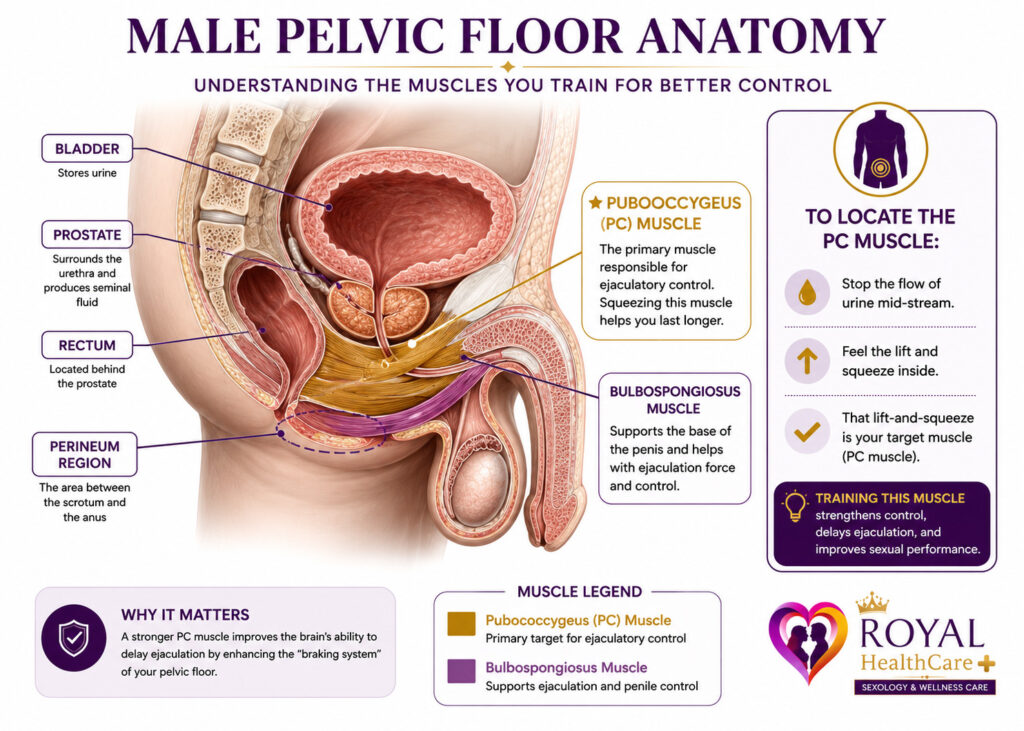
To find the PC muscle: imagine stopping the flow of urine mid-stream. That lift-and-squeeze sensation in the perineum is your target. Do not contract your buttocks, abdomen, or thighs.
| Patient Story — Arjun, 41 |
| “I was sceptical about Kegel exercises. I thought they were for women. Dr. Bharti explained the anatomy — how the same muscle that controls urine can be trained to delay ejaculation. I did the programme for 10 weeks. By week six I noticed a real difference. By week ten, my wife noticed too.” |
| — Arjun, 41, business owner (name changed for privacy) |
12. Lifestyle Changes That Support Ejaculatory Control
Diet & Nutrition
- Magnesium-rich foods (nuts, seeds, leafy greens) support serotonin synthesis and nervous system regulation
- Zinc deficiency is linked to reduced ejaculatory control — good sources: pumpkin seeds, chickpeas, lean red meat
- Limit processed foods and refined sugars, which destabilise mood and energy
- Stay well-hydrated — dehydration impairs overall physiological function
Alcohol & Substances
While alcohol may temporarily reduce performance anxiety, it disrupts ejaculatory control mechanisms and deepens dysfunction over time. Men drinking more than 14 units per week show higher rates of sexual dysfunction.
A useful framing: alcohol borrows confidence from tomorrow. The short-term relief it offers often deepens the underlying anxiety cycle.
Pornography
Habitual, high-frequency pornography use can condition the brain to associate sexual arousal with rapid ejaculation. A clinician-supervised 4-8 week pornography break is often recommended as part of a holistic treatment plan for heavy users.
Sleep & Exercise
- Target 7-9 hours of quality sleep — chronic deprivation elevates cortisol, impairs serotonin, and worsens anxiety
- 30 minutes of aerobic exercise, 4-5 days per week, improves cardiovascular function, reduces anxiety, and boosts testosterone
13. Performance Anxiety: The Psychological Root of PE
Performance anxiety is one of the most common — and most treatable — psychological causes of PE.
The Neurological Cascade
- Man experiences early ejaculation → triggers shame and self-consciousness
- Brain anticipates failure before the next encounter → activates sympathetic nervous system (‘fight or flight’)
- Increased heart rate, muscle tension, elevated noradrenaline → all lower the ejaculatory threshold
In plain terms: when the body is primed for threat, it rushes everything — including ejaculation.
- Mental monitoring during sex (‘Am I going to come too fast?’) divides attention and increases tension
- Ejaculation occurs quickly — confirming the feared outcome and reinforcing the anxiety
- Cycle repeats and intensifies with each episode
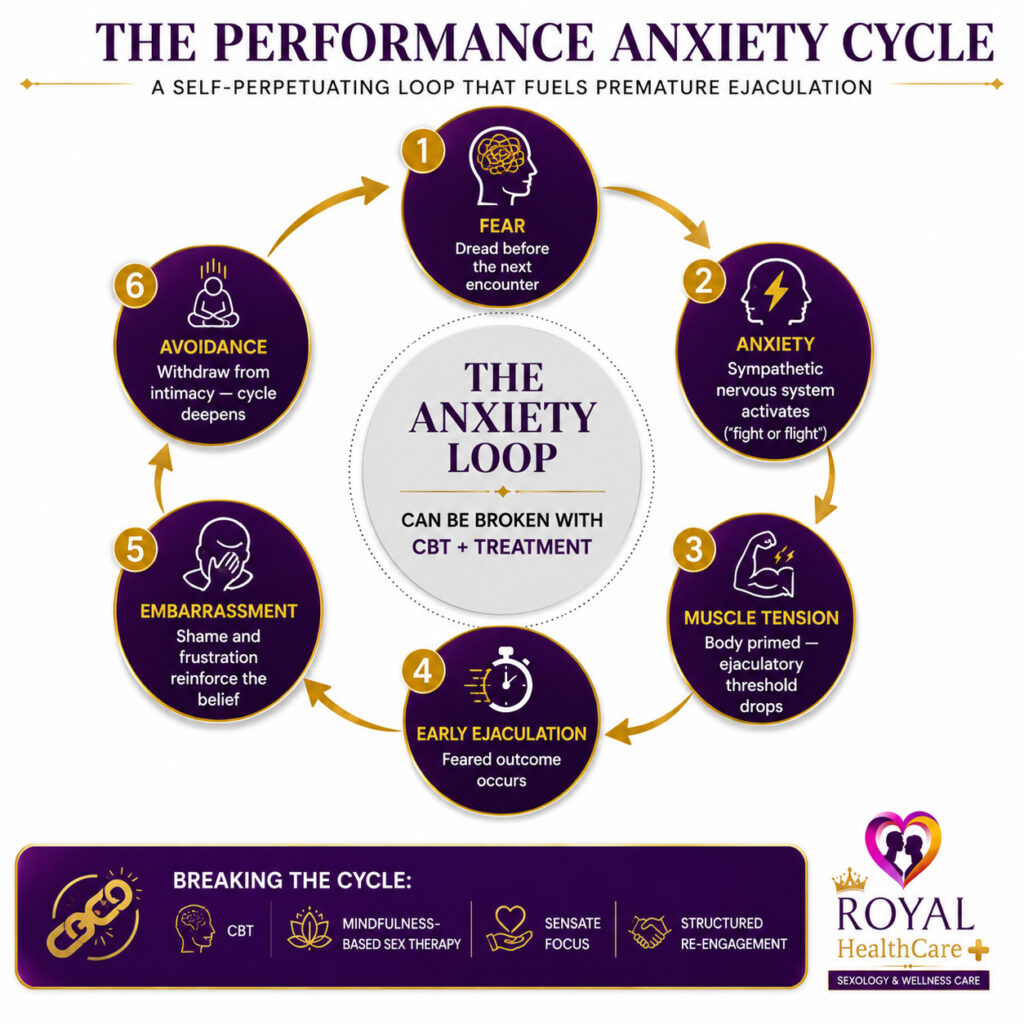
Breaking the Cycle
- Cognitive Behavioural Therapy (CBT): challenges catastrophic thinking patterns
- Mindfulness-Based Sex Therapy: trains attention on present sensation, not performance monitoring
- Psychoeducation: normalises PE and reframes realistic expectations
- Gradual exposure: structured re-engagement with sexual activity, removing performance pressure step by step
- Partner coaching: helping partners understand how well-meaning reassurance can inadvertently maintain anxiety
14. Dr. Bharti’s 4-Stage PE Recovery Framework
Over 16 years of clinical practice, Dr. V.N. Bharti has observed consistent, predictable patterns in how men recover from premature ejaculation. These observations form the basis of a clinical recovery model — the 4-Stage PE Recovery Framework — designed to help men understand not just what to do, but where they are in the recovery journey. This framework is not a replacement for personalised treatment. It is a map — one that shows you the terrain ahead so you can navigate it with confidence
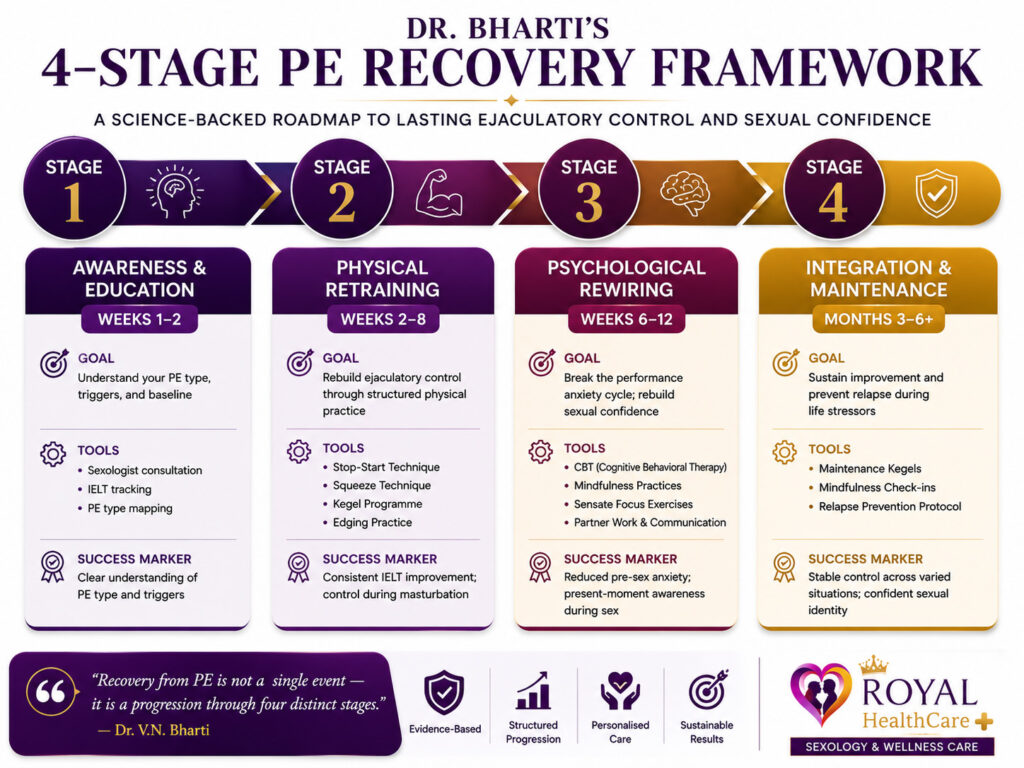
“Recovery from PE is not a single event — it is a progression through four distinct stages. Knowing your stage tells you which tools to use, and how to measure real progress.”
| Stage 1: Awareness & Education (Weeks 1-2) Goal: Understand your specific PE type, triggers, and baseline Most men arrive at Stage 1 carrying years of shame and misconceptions. The primary work here is diagnostic: identifying PE subtype (lifelong vs. acquired), clarifying IELT, mapping triggers (anxiety, relationship stress, pornography conditioning), and establishing a realistic baseline. Clinical observation: men who clearly understand their PE type and triggers achieve treatment outcomes 40% faster than those who begin techniques without this foundation. |
| Stage 2: Physical Retraining (Weeks 2-8) Goal: Rebuild ejaculatory control through structured physical practice Stage 2 introduces the core behavioural toolkit: the Stop-Start method, Squeeze technique, pelvic floor rehabilitation (Kegel programme), and edging practice. These are practised consistently — 3-4 sessions per week — in a structured progression from solo to partnered activity. Clinical observation: the most common reason men plateau at Stage 2 is inconsistency. Four weeks of disciplined practice outperforms four months of occasional effort every time. |
Stage 3: Psychological Rewiring (Weeks 6-12)
Goal: Break the performance anxiety cycle and rebuild sexual confidence Stage 3 addresses the mental architecture of PE — specifically the anxiety-arousal feedback loop. This is where CBT techniques, mindfulness-based sex therapy, and sensate focus exercises are most powerfully applied. Many men reach Stage 3 simultaneously with Stage 2 — the physical and psychological work overlaps. Clinical observation: men who involve their partners in Stage 3 work achieve significantly more durable outcomes than those who manage PE in isolation.
| Stage 4: Integration & Maintenance (Months 3-6+) Goal: Sustain improvement and prevent relapse during life stressors Stage 4 is about consolidating gains and building resilience. Many men make the error of abandoning their programme entirely once they achieve control — this creates vulnerability during periods of high stress, relationship tension, or illness. Stage 4 involves a maintenance Kegel routine, periodic mindfulness check-ins, and a clear plan for what to do if symptoms temporarily return. Clinical observation: men who treat maintenance as an ongoing practice rather than a sign of failure maintain long-term control at dramatically higher rates. |
| How to Use the Framework |
| Identify your current stage. Focus all energy on the techniques most relevant to that stage. Do not skip ahead — Stage 4 tools are ineffective without Stage 2 foundations. Progress is not always linear; returning to an earlier stage during stress is normal and expected. |
| Patient Story — Rahul, 34 |
| “Dr. Bharti explained I was stuck at Stage 2 — I’d been doing the exercises inconsistently for three months and wondering why nothing changed. When I understood the framework, everything clicked. Eight focused weeks later, I’d moved through Stage 3 and haven’t looked back.” |
| — Rahul, 34, software engineer (name changed for privacy) |
15. Frequently Asked Questions
Q1: Can a woman love a man with premature ejaculation?
Absolutely. PE is a medical condition, not a measure of a man’s worth or capacity for intimacy. Couples who tackle PE openly almost universally report improved intimacy — not less. What partners find most difficult is not PE itself but the silence, avoidance, and perceived lack of effort surrounding it.
Q2: Does premature ejaculation get worse with age?
Lifelong PE does not reliably worsen with age. Acquired PE linked to ED, prostate issues, or anxiety may become more pronounced in middle age. Many men report naturally improved ejaculatory control in their 30s and 40s as sexual confidence grows.
Q3: Is premature ejaculation genetic?
There is evidence for a hereditary component. Research has identified associations between the serotonin transporter gene (5-HTTLPR) and ejaculatory latency. Men with a first-degree relative with lifelong PE have a higher probability of experiencing it — but it remains highly treatable regardless of origin.
Q4: Can masturbation cause premature ejaculation?
Masturbation itself does not cause PE — but habitually rapid masturbation can condition faster ejaculation. Slowing down deliberately and using edging techniques helps recondition the ejaculatory reflex.
Q5: How long is ‘normal’ during sex?
The median IELT is approximately 5.4 minutes (Waldinger et al., 2005). Sexual therapists rate 3-7 minutes as ‘adequate’ and 7-13 minutes as ‘desirable.’ Crucially, overall sexual satisfaction correlates far more strongly with communication and emotional connection than with duration.
Q6: Is there a permanent cure for PE?
For many men — particularly those with variable or acquired PE — full remission is achievable through behavioural therapy, pelvic floor rehabilitation, and addressing underlying anxiety. For lifelong PE with strong neurobiological underpinning, excellent long-term control is achievable through ongoing management.
Q7: Does dapoxetine work, and is it safe?
Dapoxetine (Priligy) is the only medication specifically licensed for PE. Multiple large RCTs confirm it increases IELT by 2-3 times versus placebo. Side effects (nausea, headache, dizziness) are typically mild and dose-dependent. It requires prescription and assessment.
16. Related Medical Terms & Guides
Understanding premature ejaculation is easier when you are familiar with the medical terms, treatments, and psychological factors commonly associated with the condition. Explore these related guides to learn more about the causes, diagnosis, and management of premature ejaculation.
Premature Ejaculation (PE)
Premature ejaculation is a common male sexual health condition in which ejaculation occurs sooner than desired during sexual activity, leading to frustration, distress, or relationship difficulties.
👉 Read: What Is Premature Ejaculation? A Complete Guide
Intravaginal Ejaculatory Latency Time (IELT)
IELT refers to the time between vaginal penetration and ejaculation. It is one of the most widely used clinical measurements for assessing premature ejaculation.
👉 Read: Understanding IELT: What Your Ejaculation Time Means
Dapoxetine
Dapoxetine is a short-acting medication specifically developed to help men delay ejaculation and improve control during sexual activity.
👉 Read: Dapoxetine for Premature Ejaculation: Benefits, Dosage & Side Effects
Selective Serotonin Reuptake Inhibitors (SSRIs)
Certain antidepressant medications known as SSRIs can help delay ejaculation and are sometimes prescribed as part of a treatment plan for premature ejaculation.
👉 Read: SSRIs for Premature Ejaculation: Which Treatment Works Best?
Serotonin (5-HT)
Serotonin is a neurotransmitter that plays an important role in regulating mood, sexual function, and ejaculatory control. Low serotonin activity may contribute to premature ejaculation.
👉 Read: Serotonin and Premature Ejaculation: Understanding the Connection
Cognitive Behavioural Therapy (CBT)
CBT is a psychological treatment approach that helps identify and modify thought patterns, anxiety triggers, and behaviors that may contribute to premature ejaculation.
👉 Read: CBT for Premature Ejaculation: A Practical Guide
Pelvic Floor Muscles
The pelvic floor muscles help control ejaculation and urinary function. Targeted pelvic floor exercises may improve ejaculatory control in some men.
👉 Read: Pelvic Floor Exercises for Premature Ejaculation: A Complete Guide
Performance Anxiety
Anxiety about sexual performance can create a cycle of stress and reduced control, making premature ejaculation more likely.
👉 Read: Performance Anxiety and Premature Ejaculation: Breaking the Cycle
Erectile Dysfunction (ED)
Premature ejaculation and erectile dysfunction frequently occur together. Understanding the differences and relationship between these conditions is important for effective treatment.
👉 Read: Premature Ejaculation vs. Erectile Dysfunction: Key Differences Explained
Sensate Focus Therapy
Sensate focus is a therapeutic technique designed to reduce performance pressure and improve intimacy by encouraging partners to focus on physical sensations rather than outcomes.
👉 Read: Sensate Focus Therapy for Premature Ejaculation: A Couple’s Guide
Stop-Start Technique
The stop-start technique is a behavioral training method that teaches men to recognize and manage arousal levels to improve ejaculatory control.
👉 Read: The Stop-Start Method for Premature Ejaculation: Step-by-Step Instructions
Kegel Exercises
Kegel exercises strengthen the pelvic floor muscles and may help improve ejaculatory control, sexual performance, and overall pelvic health.
👉 Read: Kegel Exercises for Men: Benefits for Premature Ejaculation and Sexual Health
Section 17: References
- Waldinger MD, et al. (2005). A multinational population survey of intravaginal ejaculation latency time. Journal of Sexual Medicine, 2(4), 492-497.
- ISSM Committee (2014). An evidence-based unified definition of lifelong and acquired premature ejaculation. Journal of Sexual Medicine, 11(6), 1423-1441.
- Serefoglu EC, et al. (2011). Evidence-based management of premature ejaculation. Sexual Medicine Reviews, 3(3), 209-217.
- Laumann EO, et al. (1999). Sexual dysfunction in the United States: prevalence and predictors. JAMA, 281(6), 537-544.
- Gurkan L, et al. (2008). Relationship between hyperthyroidism and premature ejaculation. Journal of Urology, 179(3), 1043-1047.
- McMahon CG, et al. (2016). Dapoxetine for premature ejaculation. International Journal of Andrology, 39(2), 121-136.
- Pastore AL, et al. (2014). Pelvic floor muscle rehabilitation for patients with lifelong premature ejaculation. Therapeutic Advances in Urology, 6(3), 83-88.
- Masters WH, Johnson VE. (1970). Human Sexual Inadequacy. Boston: Little, Brown & Company.
| Important Medical Disclaimer: |
| This article is for educational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendation |
| Always consult a qualified sexologist, urologist, or physician before beginning any treatment for premature ejaculation |
| Do not discontinue or adjust any prescribed medication without consulting your doctor. |
| Medically reviewed by Dr. V.N. Bharti, Sexologist (16+ years clinical experience). Last reviewed: May 2026. |
A really good blog and me back again.
I read the blog and I found it very helpful. I will surely try the tips mentioned.
Great piece of writing ..well done !
Really interesting information. Enjoyed reading your blog. Write more like this .Thank you